IISc researchers and industry partners have developed software tools driven by AI that can complement the healthcare system in fighting COVID-19
The SARS-CoV-2 virus, which causes the disease we know as COVID-19, has kept us occupied through the first half of 2020. It is the first pandemic in a hundred years, affecting nearly every country on the planet. However, unlike previous pandemics – the Great Plague of Marseille of 1720, the Asiatic cholera pandemic around 1820, or the influenza pandemic of 1918 – we now have better tools for combating the disease. And a considerable number of these tools are driven by Artificial Intelligence, or AI.
But what does AI have to do with the efforts to combat COVID-19? AI may sound far removed from the messy world of biological viruses, but then where there’s data, there’s AI. And the COVID-19 pandemic has generated a large amount of data that can be analysed most effectively using AI.
One approach to AI is called machine learning (ML), where large amounts of data (popularly referred to as “big data”) relevant to a specific task are fed to the software program, which “learns” to analyze it using certain algorithms to solve the problem or to draw insights. In medical science, ML is already helping, for example, in identifying cancerous tumours from mammograms, diagnosing diabetic retinopathy from retinal images, and developing drugs at a lower cost. More generally, ML can help identify individuals at risk of contracting a specific disease, screen patients, predict treatment outcomes, develop effective drugs, and design the most effective diagnosis by analysing huge biomedical databases.
From a users’ point of view, ML manifests itself in drones, or smartphone apps, chatbots, and wearable sensors. In these pandemic times, the biggest USP of such applications lies in the fact that it facilitates easy screening and diagnosis of patients at home, without requiring them to come in contact with any healthcare professional.
Researchers from the Indian Institute of Science (IISc) have also been quick to see this potential. In collaboration with industry partners, they have come up with software tools driven by AI that can complement the healthcare system in fighting COVID-19.
“Go Corona Go” – no longer just a slogan
When Ramdas Athawale, the Minister of State for Social Justice and Empowerment, coined the slogan “Go Corona, Corona Go” at a rally in February, he may not have had a contact tracing app in mind. Tongue firmly in their cheeks, Yogesh Simmhan, Assistant Professor in the Department of Computational and Data Sciences (CDS), and Tarun Rambha, Assistant Professor in the Department of Civil Engineering, along with a group of PhD scholars and postdoctoral fellows, have created a contact tracing app for the IISc community and named it “GoCoronaGo”.
The idea of contact tracing is simple. Two people are said to be “in contact” if they come in close proximity to one another. Thus, you have a number of primary contacts (with whom you have been in close proximity at some point), secondary contacts (whom your primary contacts were in close proximity to after meeting you), tertiary contacts and so on. Contact tracing is a vital part of containing infectious diseases such as COVID-19, but requires laborious effort to identify and track down all the contacts of an infected person, assuming they are able to remember all the people they have met recently. This task is done by health workers or volunteers who may have to go door-to-door to track down and alert the contacts of an infected person. Smartphones with a contact tracing app installed promise to make this task easier, for one could use the proximity of the phones to one another as a proxy for their owners being in contact.
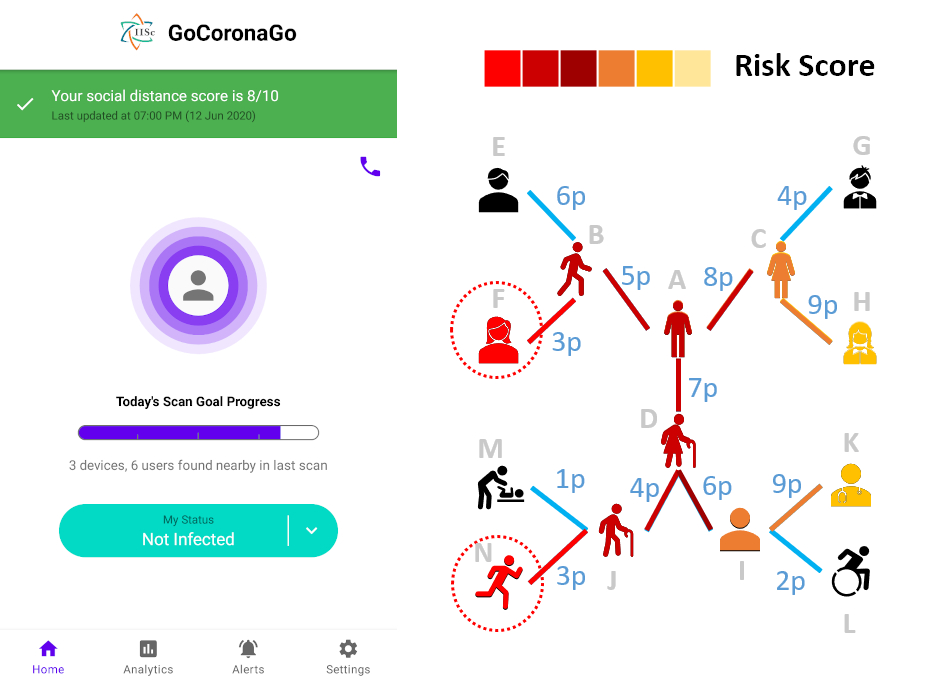
Using the list of contacts thus obtained, one can construct a “contact network” for every user of the app. If one user tests COVID-positive, the app makes it easier to quickly alert people they have recently been in contact with, helping curb the spread of the disease. “Even in the absence of any infected individuals, contact tracing helps in identifying the contacts in a network who are most vulnerable to get infected,” says Simmhan. “Usually these are the people who act as common links between two clusters of contact networks, like people who regularly travel between two isolated institutions, say, IISc and NCBS [National Centre for Biological Sciences].”
The GoCoronaGo (GCG) app is currently operational in the IISc campus with around 300 resident users, and also in NCBS. The plan is to expand the user base once the students start returning. But opening it up to the public at large in Bangalore won’t be useful. “The app is most effective when installed in a narrow spatial region with a high degree of adoption,” says Simmhan.
The GoCoronaGo app is currently operational in the IISc campus with around 300 resident users, and also in NCBS
The GCG app assigns a unique ID (randomly generated) to every device and uses Bluetooth Low Energy technology to broadcast it. This ID can be detected by GCG apps installed on other nearby devices. The app on each device keeps on broadcasting its own ID and scanning for others in its proximity. The detected IDs and the time of detection are stored in the app in the form of a virtual diary.
Similar contact tracing apps, like Aarogya Setu, TraceTogether and Safe Paths are already available and more apps are on their way. “But GCG is a bit different from the others,” says Simmhan. “Other apps store the collected data locally in the device and alert only the primary contacts in case someone tests positive. GCG, on the other hand, collects the anonymised data in a centralised database which helps to obtain far better and more useful analytics. We can identify all highly vulnerable contacts in the network and alert them by providing centralised scores as non-biological estimates of their chances of getting infected.”
GCG also tries to pro-actively nudge people towards maintaining physical distancing by sending them a “social distancing score”, which is a measure of how many new people a user comes in contact with every day. In addition, the app also sends relevant news articles and infographics from reliable science communication websites such as COVID Gyan and the Indian Scientists’ Response to COVID-19, adds Rambha.
Contact tracing apps, however, come with a burning issue: privacy. Unlike other apps, GCG doesn’t ask for any personal details. It only asks for the phone number to facilitate medical support and avoid data loss if the app is uninstalled and then reinstalled – but that too is optional. GCG also doesn’t collect GPS data unless the user gives explicit consent. “We are also working on a feature called ‘Rolling Identifier’ in which the device ID generated by the app will keep on changing after a specified period of time. So, if third-party apps try to track that ID, they will lose track of it once it changes,” adds Simmhan.
GCG’s developers have also put in place safeguards on the usage of the anonymised data the app collects. “An IISc Advisory Board including student, faculty, staff and Health Centre representatives is overseeing how we are using the collected data for operational purposes. We are also planning to get IHEC [Institute Human Ethics Committee] approval, which means a committee set up according to ICMR [Indian Council of Medical Research] guidelines will have oversight on the data collection and its use for research. We are further trying to get approval from the Government of India, as it is required for launching our app in the [Google] Playstore. The code will be made open-source in the near future,” says Simmhan.
The GCG team has launched version 0.4 of the Android app on 10 June 2020 to the initial batch of students re-entering campus. Over 250 students have downloaded and are using it, as on 12 June 2020. It will be rolled out to other students and staff over the next few weeks. A preliminary iOS version 0.1 is ready, but awaiting approval for hosting on the Apple App Store. The app is currently being reviewed by the IHEC.
The Sound of COVID – Coswara
Around the same time when GCG came to fruition, Sriram Ganapathy (Assistant Professor in the Department of Electrical Engineering) was thinking about ways to contribute to the effort to combat the pandemic. After a discussion with his colleagues and students, he realised that the symptoms of COVID-19 were mainly respiratory problems, alongside cough. Given his background in acoustics and speech processing, he decided to make a diagnostic tool based on the vocal and respiratory sounds of COVID-infected people. The name “Coswara” was an automatic choice.
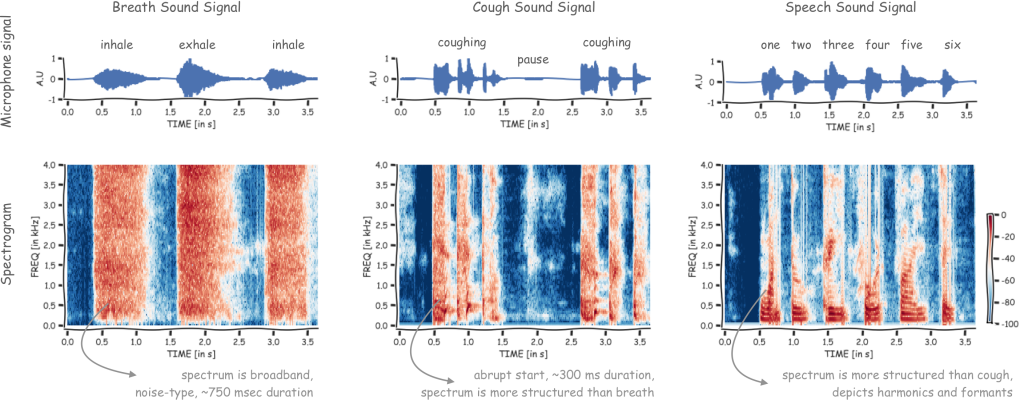
Research groups across the world have previously tried to develop diagnostic tools for treating pneumonia, asthma and other respiratory illnesses, using cough and breathing sounds of patients. “We took a closer look at their work to see if the idea could be extended for detection of COVID-19 symptoms,” says Ganapathy. “The potential scenario, in this case, would be that airflow in the respiratory system gets affected because of the infection and as a result, sounds which require strong phonation and deep breaths get distorted. We wanted to see whether we could identify the characteristics of these audio signals as potential biomarkers for this disease.”
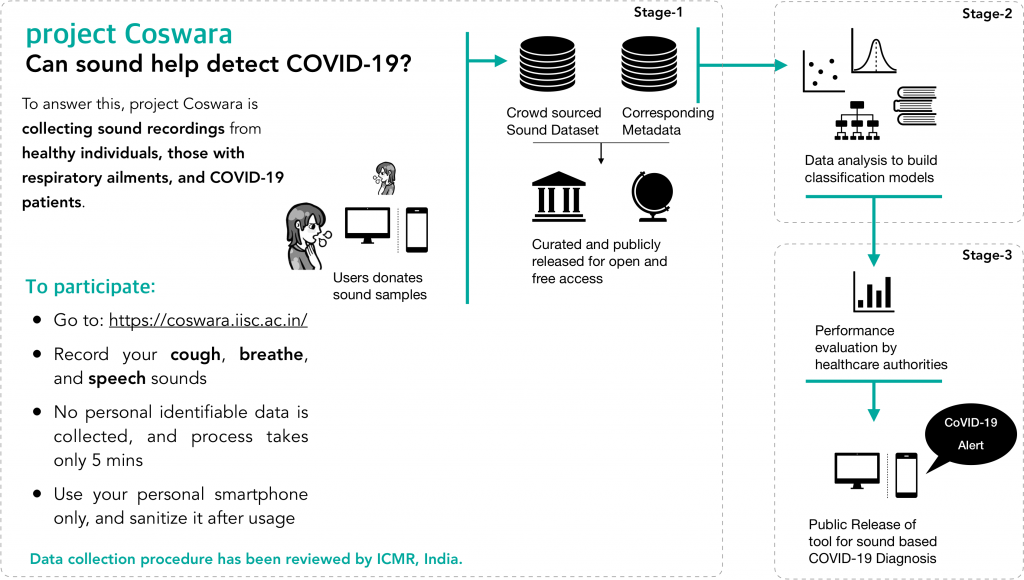
Coswara is currently collecting data through its website. The tool requires an individual to enter some personal details like age, gender and location along with any pre-existing medical history. Nonetheless, the app does not collect any personally identifiable information. The user then has to record some vocal sounds (such as pronouncing English vowels and certain consonants with and without heavy breathing) and submit these voice samples. The entire anonymised dataset, along with the voice sample, is instrumental for the ML algorithm to work efficiently and predict a risk score for the participant, indicating their chances of being infected.
So far, the Coswara app has received nearly 900 responses, mostly from Karnataka with a few from Kerala, Maharashtra and other states. Since ML efficiency depends strongly on the quantity and quality of data fed to the tool, the Coswara team believes that by late June, there might be enough data for their software to be able to detect COVID-positive users.
The audio-based diagnostic tools created by other researchers for asthma and pneumonia have reported an accuracy of about 90 percent. Recently, a study conducted in the US reported around 95 percent accuracy in detecting COVID-19 symptoms solely on the basis of audio samples of patients coughing. However, it was a small case study and involved only 50 COVID-positive subjects. “We have been in contact with groups from the UK and USA working on similar projects and have requested them to share data with us. As we get more data from COVID-19 subjects as well as those with respiratory ailments and healthy individuals, then we might be able to test and validate the hypothesis,” says Ganapathy. “The major challenge has been to reach out to a greater number of COVID-positive patients. We are now working with hospitals to enable data collection.”
The utility of this app lies in the fact that it requires only six minutes to get a rough diagnosis, without any need to visit a hospital or violate physical distancing. This may become vital in the post-COVID era, where physical distancing will still be the norm. But is the tool self-sufficient in detecting COVID-19? “We obviously don’t want people to take life-saving decisions based on the answers provided by the tool,” says Ganapathy. “The tool will act as a pre-screening mechanism. The attempt is not to replace chemical tests but to supplement them with a way to prioritise who gets tested. Given the high load on testing facilities, we believe that an AI-based simple, fast, cost-effective and contactless solution would be invaluable to the current public health system.”
Having received ICMR directive for their tool to collect data in large scales, the team now plans to collect more COVID-positive subjects’ data from government and private hospitals. The tool is currently available in six Indian languages (Hindi, Kannada, Telugu, Tamil, Marathi and Bengali). The team says that they are also in need of data from healthy individuals and subjects with pre-existing respiratory ailments. (If you would like to volunteer for the study, which takes about five minutes using a smartphone with internet access, please visit the link https://coswara.iisc.ac.in/.)
Conversations with a Chatbot about COVID-19
One drawback of ML-driven apps and technologies in real-world applications is that they require smartphones and access to the Internet. In India, at least 20 percent of people in urban areas do not own smartphones. In Pune, for example, the number of people without a smartphone is nearly 8 lakh. And an overwhelming majority of those who do not own smartphones reside in slums. These are areas where it is difficult to observe physical distancing norms and are therefore potential COVID-19 hotspots. Neither individual contact tracing nor door-to-door screening is possible in such cases. Motivated to extend medical support in such situations, Chiranjib Bhattacharyya, Professor in the Department of Computer Science and Automation (CSA), along with a team from AI Foundry, Bangalore, came forward to create a WhatsApp chatbot named CovidWATCH, where WATCH is an acronym for WhatsApp-based Assessment Through CHat.
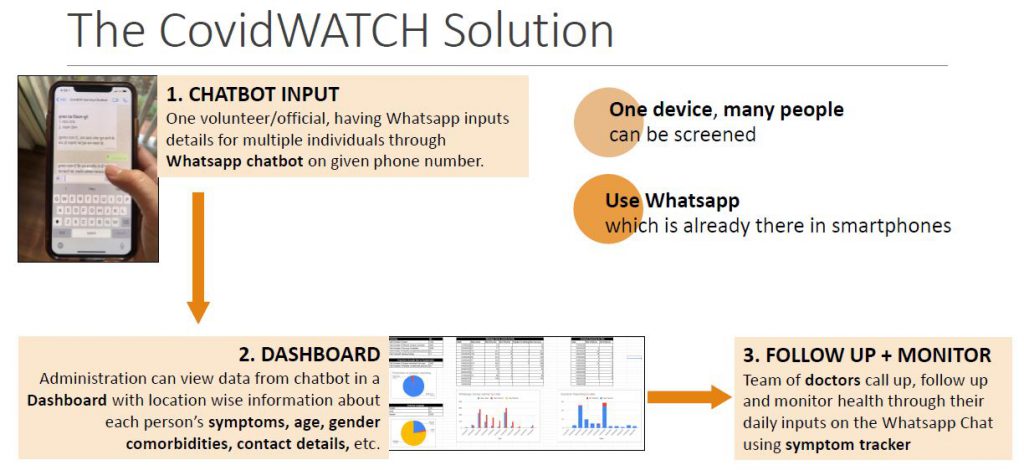
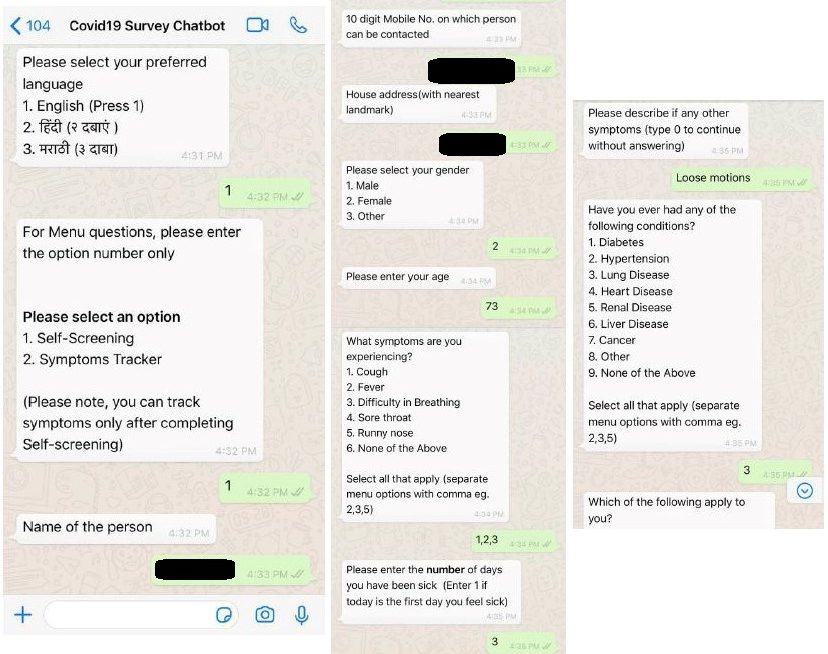
The chatbot is designed to be a quick and easy medium to alert the local civic authorities regarding any individual exhibiting “flu-like” symptoms so that the administration can arrange for their medical supervision and hospitalisation. A “survey official”, who owns a smartphone with WhatsApp installed, is appointed for a particular locality. The official communicates with the administration through a specified WhatsApp number (the chatbot) and sends information regarding any individual’s symptoms and duration of sickness, by answering a list of questions provided by the chatbot. The questions can be answered multiple times for entering information about multiple people residing in that locality, using the same WhatsApp account. The information is viewed by a team of doctors who follow up with the official by phone call and prescribe the next steps for each patient. The official can update a patient’s symptoms regularly through the chatbot, which enables the doctors to diagnose them properly.
“Unlike prevalent contact tracing apps, CovidWATCH does not require installation of any additional app and a single device can cater to multiple patients. It can be leveraged as a survey tool,” says Bhattacharyya. “The bot is also capable of multilingual chats.”
Currently, the tool is being used by the Pune administration for surveying COVID-19 hotspot areas in the city. “The Pune police have employed 1,400 residents of various slums to survey their own neighbourhoods. Till now, nearly 4,000 individuals have been surveyed by them,” says Nabanita Paul, one of Bhattacharyya’s PhD students. “The Pune Municipal Corporation has engaged a team of doctors and they are in constant touch with these volunteers. From May 29 onwards, the Pune Police is also strictly monitoring their own force using the chatbot.”
The team plans to upgrade the chatbot based on the feedback received from users and administrations. “From a self-screening tool for public use, to a tool for surveys in slums, enabling quick administrative response, to now self-reported daily mandatory screening in the police force, it has evolved in a need-based fashion,” says Niharika Venkatesh of AI Foundry.
The Future of AI in healthcare
AI is still perceived by many as an out-of-the-world futuristic concept, and sometimes this leads to unrealistic expectations about AI which can never be fulfilled. All contact tracing methods, for example, are prone to false alarms, and crowd-sourced data can generate erroneous results. No ML-based application can be perfect, but that does not nullify their importance.
“This is probably the first large pandemic that we have seen, but it certainly won’t be the last one that we will see in our lifetime,” says Simmhan. “It is going to be like an annual event, and maybe every five years you will get something even more virulent. So, the quicker we researchers adapt to the situation and find solutions to this problem, the more functional we can be and the more we can go about our daily lives without getting affected by this.” And how do AI-based apps figure in this grand scheme of things? “This might just become the new normal, where you assume that there is going to be some backend analytics involving your contact data which will keep you safe (and your data confidential), and you slowly start to rely on contact tracing,” he says.
Such tools, as CovidWATCH shows, can be useful not just for individuals, but also for civic administrations. “Apart from individual health care, the pandemic has also drawn our attention to the need for community-based disease surveillance,” says Bhattacharyya. “Tech adoption for addressing this issue is the need of the hour and our chatbot is a nano-step in that direction.” Ganapathy has a similar vision. “Healthcare experts are already in favour of using these apps in order to facilitate remote diagnostics,” he says. “This will surely benefit the growth of telemedicine technologies in future. And every country including India is going to prefer contactless testing of various respiratory disorders, even when the pandemic situation is over.”
Aniket Majumdar, a second-year Integrated PhD student in the Department of Physics, is a science writing intern at the Office of Communications.
For more stories about the COVID-19 crisis, click on the links below:
Tracking the Scourge: Diagnostics, Testing and Vaccines for COVID-19
Engineering Our Way Out of the COVID-19 Crisis
The Pandemic and Mental Health at IISc
Understanding COVID-19 Through the Lens of the Social Sciences